Location & Hours
4008 Red Cedar Dr D-1
Highlands Ranch, CO 80126-8152
| Mon & Fri: | 8 - 4 |
| Tues - Thurs: | 10 - 7 |

Shingles is the term we use to describe a condition that is caused by a re-activation of the Herpes Varicella-Zoster virus. The origin of this infection usually goes way back to childhood with a disease we know as chickenpox.
When you have a chickenpox infection your immune system manages to eventually suppress that virus from causing an active infection, but the virus does not get completely eliminated from your body--it is able to go and hide in your nerve roots.
Your immune system manages to keep the virus in check for most of your life but there may come a time in adulthood when your immune system is not working as well as it used to, and the virus can reappear. It usually does this along the distribution of a single sensory nerve called a dermatome.
The most common area for this to occur is along your trunk (chest or abdomen) but it is also commonly found on the face.
There are three branches of nerves that supply sensation to your face. They are all branches of the fifth cranial nerve. Those three branches supply the upper face (V1), the mid face (V2), and the lower face (V3). Most of the time, shingles breaks out along only one of the branches at a time. The one that most frequently involves the eye is a rash breakout in the V1 distribution. This can involve the forehead and both the upper and lower eyelid. It is also much more likely that the inside of the eye will be involved if the tip of the nose has a lesion on it. The reason for that is that there is a specific subbranch of the V1 nerve called the nasocilliary nerve. This nerve is responsible for sensation on the tip of the nose and the inside of the eye.
The hallmark of shingles is that once the rash erupts it stays on one side of the body, including when it happens on the face. The rash will go up to the centerline of your face but will not go to the other side. You may get lesions on your scalp, but they will not show up on the back of your head. That is because the V1 does not go past half way back on your scalp. The back of your head has its sensation handled by nerves that come out of your spinal cord not cranial nerves that come out of the front of your skull.
Many people have a hard-to-describe sensation of pain, irritation, or itching along the distribution of the nerve for a day or two before the rash shows up. It is important to recognize the rash as quickly as possible because the drugs that treat shingles--usually Acyclovir, Famvir (famciclovir), or Valtrex (valacyclovir)--are much more effective if they are started within three days of the beginning of the rash.
Eye problems may occur along with the rash, especially if there is a lesion on the tip of the nose.
The two biggest problems are swelling or inflammation of the cornea and inflammation inside the eye, which we call iritis or uveitis.
The inflammation in the eye can cause pain and it can also increase eye pressure and cause glaucoma. Most often the treatment for the eye problem is to use the same oral medication mentioned above and sometimes it also can require eye drops to decrease the inflammation the virus is causing (steroid drops) or drops to try and lower the elevated pressure (glaucoma drops).
The eye inflammation can cause blurred vision, pain, and significant light sensitivity. It can be hard to treat and control and can continue to be a problem long after the skin lesions are gone. In fact, many times problems don’t even start until the skin lesions are starting to go away.
It is recommended that if you have shingles affecting the distribution of V1, you should have an eye exam within a few days of the diagnosis being made and then another exam again a week later because, as mentioned above, the eye problems can present a week later than the skin eruptions.
There can be some serious long-term effects of shingles on your eye, including glaucoma and corneal scarring that can be bad enough to require a corneal transplant. The symptoms are often obvious with the vision being blurry and the eye being very red and painful, but sometimes the symptoms may be much more mild even when significant trouble is brewing inside the eye. So even if you think the eye feels fine, you need an exam to ensure there is not subtle inflammation or significant elevation of the pressure in the eye.
The other long-term problem with shingles around the eye is the possibility of there being ongoing pain in the area that can last for many years. This is called Post Herpetic Neuralgia (PHN). This pain can occur all along the dermatome where shingles had occurred. The eye itself may look perfectly normal but the pain persists. This is often treated with drugs that were originally developed as seizure medication but have since been shown to help alleviate neurological pain. The two most commonly used drugs for this are Neurontin (Gabapentin) and Lyrica (Pregabalin).
The most important thing you can do to try and make sure this doesn’t happen to you is to be vaccinated for shingles. The original vaccination called Zostavax has been available since 2006 in the U.S. It is a single-injection vaccine and was recommend for everyone over 60. The main issue with this vaccine is that it only reduced the risk of getting shingles by 51% and PHN by 67%. In 2017 a new vaccine was approved in the U.S. called Shingrix. This vaccine is a two-injection vaccine with the second shot given 2 to 6 months after the first. This vaccine is recommended for everyone 50 years or older. The big advantage of this vaccine is that is 85-97% effective in preventing both shingles and PHN in people with normal immune systems. For more information about this vaccine you can go to the CDC website by clicking here.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Your Eyes Are A Precious Gift--Protect Them During The Holidays
“I want an official Red Ryder, carbine action, two-hundred shot range model air rifle!”
“No, you'll shoot your eye out.”
This line from “A Christmas Story” is one of the most memorable Christmas movie quotes ever. Funny in the movie, but the holiday season does present a real eye injury threat.
For those who celebrate Christmas, that risk begins even before the actual day.
Some of the most frequent holiday-related eye injuries come from the Christmas tree itself.
Holiday eye safety begins with the acquisition of the tree. If you are cutting down your own tree, please wear eye protection when doing the cutting--especially if you are going to be using a mechanical saw, such as a chain saw or sawzall. You need to also be careful of your eyes when loading a tree on top of the car. It is easy to get poked in the eye when heaving the tree up over your head.
Once back at home, take care to make sure no one else is standing close to the tree if you had it wrapped and now need to cut the netting off. The tree branches often spring out suddenly once the netting is released.
Other injuries occur in the mounting and decorating phase. Sharp needles, pointy lights, and glass ornaments all pose significant eye injury risk. If you are spraying anything like artificial tree snow on the branches be sure to keep those chemicals out of your eyes.
Having now successfully trimmed the tree without injury, let’s move our holiday eye safety talk to the toys.
We want to spend the holiday happily exchanging gifts in front of a warm fire, drinking some eggnog, and snacking on cookies--not going to the emergency room with an injury.
The Consumer Product Safety Commission reported there were 254,200 toy-related emergency room visits in 2015, with 45% of those being injuries to the head and face--including the eyes.
In general, here are the recommendations from the American Academy of Ophthalmology in choosing eye-safe toys for gifts:
- “Avoid purchasing toys with sharp, protruding or projectile parts."
- “Make sure children have appropriate supervision when playing with potentially hazardous toys or games that could cause an eye injury."
- “Ensure that laser product labels include a statement that the device complies with 21 CFR (the Code of Federal Regulations) Subchapter J."
- “Along with sports equipment, give children the appropriate protective eyewear with polycarbonate lenses. Check with your eye doctor to learn about protective gear recommended for your child's sport."
- “Check labels for age recommendations and be sure to select gifts that are appropriate for a child's age and maturity."
- “Keep toys that are made for older children away from younger children."
- “If your child experiences an eye injury from a toy, seek immediate medical attention.”
More specifically, there is a yearly list of the most dangerous toys of the season put out by the people at W.A.T.C.H. (world against toys causing harm).
Here are types of toys to avoid:
- Guns that shoot ANY type of projectile. This includes toy guns that shoot lightweight, cushy darts.
- Water balloon launchers and water guns. Water balloons fired from a launcher can easily hit the eye with enough force to cause a serious eye injury. Water guns that generate a forceful stream of water can also cause significant injury, especially when shot from close range.
- Aerosol string. If it hits the eye it can cause chemical conjunctivitis, a painful irritation of the eye.
- Toy fishing poles. It is easy to poke the eyes of nearby children.
- Laser pointers and bright flashlights. The laser or other bright lights, if shined in the eyes for a long enough time, can cause permanent retinal damage.
There are plenty of great toys and games out there that pose much lower risk of injury so choose wisely, practice good Christmas eye safety, and have a great holiday season!
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
There is a common misconception that any adverse reaction to a drug is an allergy. That is definitely not the case.
Reporting to your doctors that you have an allergy to a medication when what you really had was a side effect could potentially create a substantial alteration to your medical care in the future. And this could mean a physician might avoid using a drug that could possibly save your life because of the fear of an allergic reaction.
An anaphylactic allergic reaction generally produces a very specific set of symptoms, including difficulty breathing due to constriction of windpipe, swelling of your tongue, and/or a rash and hives that break out over your body. While an allergic reaction can present in other ways, these are the most frequent reactions that occur when you have a true allergy to something.
If that is not the type of reaction you had then it probably isn’t an allergy. If you are uncertain if your reaction to a medication is an allergy or not, testing by an allergist may be able to tell you if your reaction was a true allergy or a side effect.
It is not always just the patient who can misdianose a side effect as an allergy. Sometimes it is the doctor or the dentist who tells the patient, “You must be allergic.” This is a quick and easy explanation but not always the correct one.
In optimal medicine, there are not always a lot of “lifesaving” incidences, but there are several drugs that are the preferred treatment for certain conditions and if you report an allergy to these drugs it may make your doctor use a much less effective drug.
Here are some specific examples of when a false report of an allergy may lead to less effective treatment or even failure to offer life-saving treatment.
Epinephrine
The most common potential “lifesaving” drug to which patients sometimes report an allergy to is Epinephrine.
The story usually goes something like this: “I was having a dental procedure and soon after the dentist injected my mouth with a local anesthetic of lidocaine with epinephrine my heart started racing and pounding out of my chest and I almost passed out.” This hypothetical patient may come to the conclusion or the dentist may mention that the patient is allergic to epinephrine. That reaction is almost never an allergy but a side effect that occurs when a substantial dose of the lidocaine and the epinephrine gets into the blood stream and stimulates the heart.
The mouth and gums are very vascular, and it is easy to have some of that injection end up in the bloodstream, but that reaction is not an allergy and should not be reported as such.
Epinephrine is used to treat severe (anaphylactic) allergic reactions and not using it if you were to ever have a severe allergic reaction could lead to some very bad outcomes. This is not to say you can’t be allergic to epinephrine. You can, but it is extremely rare. If there is any doubt you should be tested by an allergist before you ever record yourself in a medical setting as being “allergic” to epinephrine.
Cortisone/Steroids
Cortisone is a highly effective drug to treat many conditions. Again, it is unlikely but not impossible to be allergic to it.
We all have naturally occurring cortisol circulating in our bodies and cortisone is a very similar molecule but not exactly the same. Cortisone also can have a wide range of side effects depending on where and how it is administered
Some of the common side effects of cortisone, which have been mislabeled as an allergy, are: Making your blood sugar rise, insomnia, mood swings, nausea, and weight gain. These are all known side effects of the drug and not allergies. Cortisone side effects are associated with only certain routes of administration and are often dose dependent.
Why is this important in terms of your eye care? We often use cortisone derivatives, like Prednisolone, to fight inflammation that may occur in your eye, particularly after any ocular surgery. If you report that you are allergic to cortisone when you really only experienced a side effect, we are going to have to use a less-effective medication to deal with your eye inflammation.
As I mentioned above, most side effects are dose dependent and the dose you got in a pill may have caused a side effect you’d rather not have again but the dose in an eye drop is significantly less and highly unlikely to give you the side effect you got with a pill taken orally.
Antibiotics
People often report they are allergic to antibiotics when they really experienced a side effect.
The most common side effect with oral antibiotics is some type of gastrointestinal disturbance, like nausea, or diarrhea. If that was what you had and just prefer not to get that again you still shouldn’t report it as an allergy. If you do, then the drug can’t be used as an eye drop or ointment that might be the best treatment for your condition.
An antibiotic eye drop/ointment is very unlikely to produce the same gastrointestinal trouble that the same antibiotic gave you when given as a pill. You don’t want to take away the most effective treatment for your problem because you mislabeled a side effect as an allergy.
Sedatives/Anesthesia
Most of the time with these drugs the issue is how you felt either during or after a procedure.
Common comments are “it took me too long to wake up” (side effect not an allergy); “the sedative I got in my IV burned when it went in” (side effect not an allergy); “I was sleepy all day” (side effect not an allergy); “I was nauseous after the procedure” (could be an allergy but much more likely to be a side effect).
Why are these important? We can make you much more comfortable for a local anesthesia procedure if we can use some sedation. Using sedation may be better for you and the doctor performing the surgery because you are much less likely to move during the surgery if you are resting comfortably.
If you ever have an untoward reaction to a medication it is worth your time and effort to really probe into the issue to figure out if what you had was really an allergy or just a side effect because sometimes your life may depend on it.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

There are certain eye conditions where an injection into your eye might be recommended.
Injections into the eye, specifically into the vitreous or gel-filled cavity of the eye, are called intravitreal injections.
In Part 1 of "You Want to Do WHAT to My Eye?" we talked mostly about anti-vascular endothelial growth factor (anti-VEGF) injections. Anti-VEGF injections are probably the most commonly injected agents and they are used to treat wet age-related macular degeneration (ARMD), diabetic retinopathy, and retinal vein occlusion.
But there are other injections that may be used as treatment.
Another injected medication used in combination with Anti-VEGF agents to treat wet macular degeneration, diabetic retinopathy and retinal vein occlusion are steroids. Additionally, steroids can be used to treat inflammation, or uveitis, in the eye. There is a steroid implant called Ozurdex, that looks like a white pellet and can last up to 3 months in the eye. The downside of steroids is that they can increase eye pressure and cause progression of cataracts.
Antibiotics are another type of medication that can be injected into the eye. Sometimes an infection called endophthalmitis can develop inside the eye. This can occur after eye surgery or a penetrating injury to the eye. The presenting signs and symptoms of endophthalmitis are loss of vision, eye pain and redness of the eye. Bacteria is usually the cause of the infection, and antibiotics are the treatment. The best way to deliver the antibiotics is to inject them directly into the eye.
Another relatively new injection is Jetrea, an enzyme that breaks down the vitreous adhesions that may develop on the surface of the retina. As we age, the vitreous contracts away from the retinal surface. When this occurs over the macula, the region responsible for fine vision, the result is visual distortion. Jetrea is an injection that will dissolve the vitreous adhesions and relieve the traction on the retina. Prior to the advent of Jetrea, the only treatment would have been surgery to physically remove the vitreous jelly and traction on the retina.
The next time you visit your eye doctor and are told you need an injection of medication, it will likely be one of the above agents.
Article contributed by Dr. Jane Pan

There are some eye conditions where your doctor might recommend an eye injection as a treatment option.
Injections into the eye, specifically into the vitreous or gel-filled cavity of the eye, are called intravitreal injections.
Anti-vascular endothelial growth factors (anti-VEGF) are probably the most commonly injected agents. They are used to treat wet age-related macular degeneration (ARMD), diabetic retinopathy, and retinal vein occlusion.
In these conditions, there are abnormal leaky blood vessels that cause fluid and blood to accumulate in and under the retina. This accumulation of fluid results in loss of central vision. The role of anti-VEGF agents is to shrink these abnormal vessels and restore the normal architecture of the retina.
Three anti-VEGF agents that are widely administered are Lucentis, Avastin, and Eylea.
Lucentis (Ranibizumab) is FDA approved for treatment of wet ARMD, diabetic retinopathy, and vein occlusion. It is specially designed for injection into the eye and is a smaller molecule than Avastin so it may have better penetration into the retina.
Avastin (Bevacizumab) was originally approved by FDA for treating colorectal cancer. It is used “off-label” for the same treatment indications as Lucentis. Off-label usage of medication is legal, but pharmaceutical companies can't promote a medication for off-label use. The amount of Avastin needed for eye injections is a fraction of the amount used to treat colorectal cancer, therefore, the cost of ophthalmic Avastin is only a fraction of the cost of Lucentis. This means that Avastin needs to be prepared sterilely into smaller doses by an outside pharmacy prior to injection into the eye.
Eylea (Aflibercept) is the third anti-VEGF agent. It was designed to have more binding sites than Avastin and Lucentis so it may last longer in the eye than the former two. Eylea is FDA approved for treatment of wet ARMD, diabetic disease, and vein occlusion, and therefore, the cost of Eylea is similar to the cost of Lucentis.
There are also newer agents on the market. Your doctor will deterine which might work best for you.
There is a thought that after prolonged injections, some patients may develop resistance to one particular agent but still respond to the a different agent. Therefore, your ophthalmologist will individualize your treatment.
Article contributed by Dr. Jane Pan

One of the most commonly asked questions in an eye exam comes right after the refraction, or glasses prescription check: “What is my vision?”
Almost invariably, people know the term “20/20”. In fact, it’s a measure of pride for many people. “My doctor says I have 20/20 vision.” Or, on the other side of that same coin, having vision that is less than 20/20, say 20/400, can be a cause of great concern and anxiety. In this discussion I will describe what these terms actually mean.
To lay the foundation, let’s discuss some common terms. Visual acuity (VA) is clarity or sharpness of vision. Vision can be measured both corrected (with glasses or contact lenses) and uncorrected (without glasses or contact lenses) during the course of an eye exam. The result of an eye exam boils down to two different but related sets of numbers: your VA and your actual glasses prescription.
The notation that doctors use to measure VA is based off of a 20-foot distance. This is where the first 20 in 20/20 comes from. In Europe, since they use the metric system, it is based on meters. The 20/20 equivalent is 6/6 because they use a 6-meter test distance. The second number is the smallest line of letters that a patient can read. In other words, 20/20 vision means that at a 20-foot test distance, the person can read the 20/20 line of letters.
The technical definition of 20/20 is full of scientific jargon - concepts such as minutes of arc, subtended angles, and optotype size. If you’d like to read more of the technical details there is a well-written article with illustrations by Dr. John Ellman, you can find here. For the purposes of our discussion here I’ll try to explain it in less technical terms.
“Normal” vision is somewhat arbitrarily set as 20/20 (some people can see better than that). Let’s say you have two people: Person A with 20/20 vision and Person B with 20/40 vision. The smallest line of letters that person B can see at 20 feet is the 20/40 line. Person A, with “normal” 20/20 vision, could stand 40 feet away from that same line and see it. There is somewhat of a linear relationship in that the 20/40 letters are twice the size of the 20/20 letters and someone with normal vision could see a 20/40 letter at twice the distance as the person with 20/40 vision.
So how does this translate to a glasses prescription?
Eye doctors can often estimate what your uncorrected VA will be based on your glasses prescription. This works mainly for near-sightedness. Essentially, every quarter step of increasing glasses prescription (i.e. -1.25 as compared to -1.50) means a person can see one less line on a VA chart.
A prescription of - 1.25 works out to roughly 20/50 vision, -1.50 to 20/60 and so on. Anybody with an anatomically sound eyeball, meaning the absence of any kind of disease process, should generally be correctable to 20/20 with glasses or contact lenses. It is important to note, however, that rarely a person’s best corrected VA may be less than 20/20 with no noticeable signs of disease.
Far-sightedness is more difficult to estimate because it is affected by a number of other factors, including one’s age and focusing ability. But that’s a topic for another article.
So there you have it! Hopefully this has shed some light on what these measurements that we take actually mean, and it has allowed you to understand your eye health a little bit better.
Article contributed by Dr. Jonathan Gerard
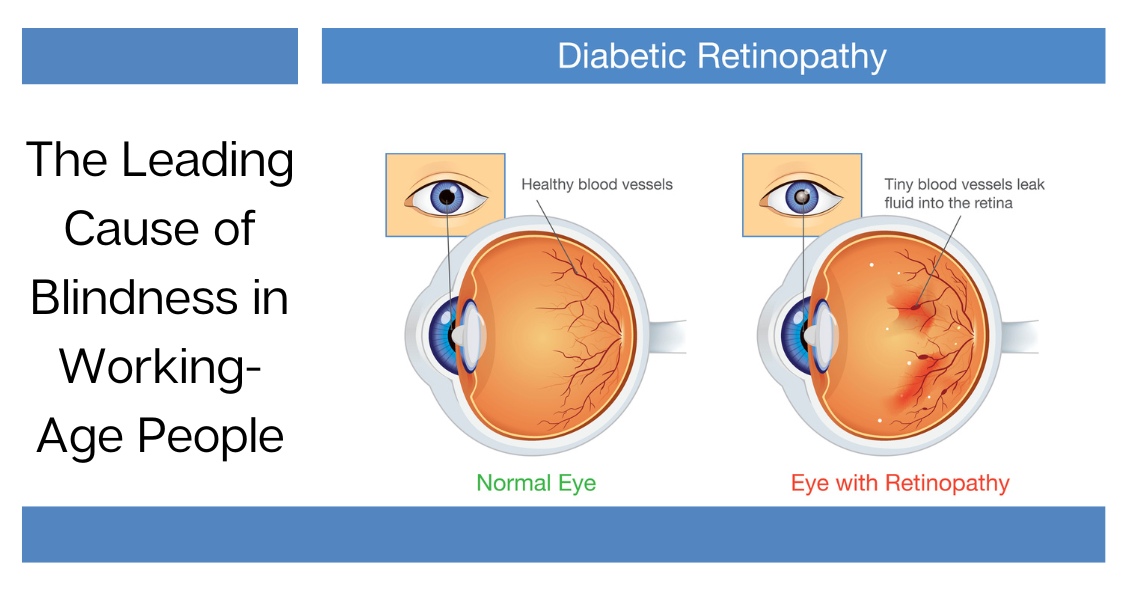
Diabetic retinopathy is an eye condition that can affect the retina of people who have diabetes.
The retina is the light-sensitive tissue that lines the back of the eye, and it detects light that is then processed as an image by the brain. Chronically high blood sugar or large fluctuations in blood sugar can damage the blood vessels in the retina. This can result in bleeding in the retina or leakage of fluid.
Diabetic retinopathy can be divided into non-proliferative or proliferative diabetic retinopathy.
Non-proliferative diabetic retinopathy: In the early stage of the disease, there is weakening of the blood vessels in the retina that causes out-pouching called microaneurysms. These microaneurysms can leak fluid into the retina. There can also be yellow deposits called hard exudates present in the retina from leaky vessels.
Diabetic macula edema is when the fluid leaks into the region of the retina called the macula. The macula is important for the sharp central vision needed for reading and driving. The accumulation of fluid in the macula causes blurry vision.
Proliferative diabetic retinopathy: As diabetic retinopathy progresses, new blood vessels grow on the surface of the retina. These blood vessels are fragile, which makes them likely to bleed into the vitreous, which is the clear gel that fills the middle of the eye. Bleeding inside the eye is seen as floaters or spots. Over time, scar tissue can then form on the surface of the retina and contract, leading to a retinal detachment. This is similar to wallpaper contracting and peeling away from the wall. If left untreated, retinal detachment can lead to loss of vision.
Symptoms of diabetic retinopathy:
- Asymptomatic: In the early stages of mild non-proliferative diabetic retinopathy, the person will usually have no visual complaints. Therefore, it is important for people with diabetes to have a comprehensive dilated exam by their eye doctor once a year.
- Floaters: This is usually from bleeding into the vitreous cavity from proliferative diabetic retinopathy.
- Blurred vision: This can be the result of fluid leaking into the retina, causing diabetic macular edema.
Risk factors for diabetic retinopathy:
- Blood sugar. Lower blood sugar will delay the onset and slow the progression of diabetic retinopathy. Chronically high blood sugar and the longer the duration of diabetes, the more likely chance of that person having diabetic retinopathy.
- Medical conditions. People with high blood pressure and high cholesterol are at greater risk for developing diabetic retinopathy.
- Ethnicity. Hispanics, African Americans, and Native Americans are at greater risk for developing diabetic retinopathy.
- Pregnancy. Women with diabetes could have an increased risk of developing diabetic retinopathy during pregnancy. If they already have diabetic retinopathy, it might worsen during pregnancy.
Article contributed by Jane Pan M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
A refraction is a test done by your eye doctor to determine if glasses will make you see better and what your prescription is.
The charges for a refraction are covered by some insurances but not by all.
For example, Medicare does not cover refractions because they consider it part of a “routine” exam and Medicare doesn’t cover most “routine” procedures--only health-related procedures.
So if you have a medical eye problem like cataracts, dry eyes, or glaucoma then Medicare and most other health insurances will cover the medical portion of the eye exam but not the refraction.
Some people have both health insurance--which covers medical eye problems--and vision insurance--which covers “routine” eye care (no medical problems) such as refractions and eyeglasses.
If you come in for a routine exam with no medical eye problems or complaints and you have a vision plan, then the refraction is usually covered by your vision insurance.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

The tears that coat the surface of your eyes have both a liquid and a mucous layer to them. It is normal to have a small amount of mucus in your tear film. But that mucus can significantly increase when the eye gets irritated.
Some of the most common causes of irritation that can make the eye overproduce mucus are:
- Conjunctivitis, which could be caused by an allergy, bacteria, or virus
- Blepharitis, which is an inflammation of the eyelids
- Dry Eye Syndrome
When any of these conditions occur, the eye will begin to make more mucus.
Sometimes the mucous production really is excessive and there is a temptation to keep pulling it out with either your fingers or a cotton swab. DON'T DO THIS--it will just lead to recurring irritation and problems.
Any mucus that gets deposited OUTSIDE the eye on the outer eyelid or on the lashes is fair game for removal. In fact, anything on the exterior of the eyelid or stuck to the eyelashes should be cleaned off. Just don’t reach INSIDE the eyelids.
Every time you go inside the eye to remove mucus, your finger or a cotton swab further irritates the eye and causes it to make even more mucus and you end up with the viscious cycle that we call mucus fishing syndrome.
If you have an acute problem that is causing excessive mucus, you need to try and get the underlying problems treated and under control. That means treating the allergy, blepharitis, infectious conjunctivitis, or dry eye syndrome.
In addition, you need to STOP putting your fingers in your eye and pulling the mucus out. Sit on your hands if you have to--but you have to stop or it is never going to get better.
If you have gone through treatment for the original problem but still find yourself pulling mucus out of your eye, you may need your doctor to try a steroid drop in order to decrease the production and try to help you get out of the habit of putting your fingers in your eyes.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

A wrinkle on the retina -- which is also known as an epiretinal membrane (ERM) or a macular pucker -- is a thin, translucent tissue that develops on the surface of the retina.
The retina is the inner layer that lines the inside of the back of the eye and is responsible for converting the light image into an electrical impulse that is then transmitted to the brain. An epiretinal membrane that forms on the retina goes unnoticed by the patient many times, and is only noticed during a dilated eye exam by an eye doctor.
Epiretinal membranes can become problematic if they are overlying the macula, which is the part of the retina that is used for sharp central vision. When they become problematic they can cause distortion of your vision, causing objects that are normally straight to look wavy or crooked.
Causes of a wrinkle on the retina
The most common cause is age-related due to a posterior vitreous detachment, which is the separation of the vitreous gel from the retina. The vitreous gel is what gives the eye its shape, and it occupies the space between the lens and the retina. When the vitreous gel separates from the retina, this can release cells onto the retina's surface, which can grow and form a membrane on the macula, leading to an epiretinal membrane.
ERMs can also be associated with prior retinal tears or detachments, prior eye trauma, or eye inflammation. These processes can also release cells onto the retina, causing a membrane to form.
Risk factors
Risk for ERMs increases with age, and males and females are equally affected.
Both eyes have ERMs in 10-20% of cases.
Diagnostic testing
Most ERMs can be detected on a routine dilated eye exam.
An optical coherence tomography (OCT) is a noninvasive test that takes a picture of the back of the eye. It can detect and monitor the progression of the ERM over time.
Treatment and prognosis
Since most ERMs are asymptomatic, no treatment is necessary. However, if there is significant visual distortion from the ERM or significant progression of the membrane over time, then surgical intervention is recommended. There are no eye drops, medications, or nutritional supplements to treat or reverse an ERM.
The surgery is called a vitrectomy with membrane peeling. The vitrectomy removes the vitreous gel and replaces it with a saline solution. The epiretinal membrane is then peeled off the surface of the retina with forceps.
Surgery has a good success rate and patients in general have less distortion after surgery.
Article contributed by Dr. Jane Pan
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Fall brings a lot of fun, with Halloween playing a big part in that.
But did you know that some Halloween practices could harm your vision? Take Halloween contacts, for instance. Costume contacts vary widely, with everything from monster eyes to goblin eyes to cat eyes to sci-fi or glamour looks. They can be just the added touch you need for that perfect costume. However, some people do not realize that the FDA classifies contact lenses as medical devices that can alter cells of the eye and that can damage the eye if they are not fit properly.
Infection, redness, corneal ulcers, hypoxia (lack of oxygen to the eye) and permanent blindness can occur if the proper fit is not ensured. The ICE, FTC, and FDA are concerned about costume contacts from the illegal black market because they are often unsafe and unsanitary. Proper safety regulations are strictly adhered to by conventional contact lens companies to ensure that the contact lenses are sterile and packaged properly and accurately.
Health concerns arise whenever unregulated black-market contacts come into the US market and are sold at flea markets, thrift shops, beauty shops, malls, and convenience stores. These contacts are sold without a prescriber's prescription, and they are illegal in the US. There have also been reports of damage to eyes because Halloween spook houses sometimes ask employees to share the same pair of Halloween contact lenses as they dress up for their roles.
So the take home message is, have a great time at Halloween, and enjoy the flare that decorative contacts can bring to your costume, but get them from a reputable venue using a proper legal prescription. Don't gamble with your eyes for a night of Halloween fun!
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

The eye care medical field has an unusual split between two different types of insurance for covering eye issues: health insurance and vision insurance. Not all patients have both.
In most cases, your health insurance is used to cover medical and surgical eye problems but not routine exams or the cost of contacts or glasses. Those things are often covered by separate vision insurance.
Why the difference? Originally, health insurance was created to take care of health “problems” and wasn’t designed to cover “routine,” “screening,” or “wellness” exams.
Since health insurance wasn’t going to cover “routine” eye exams, the vision insurance industry arose to help insure/cover those routine exams as well as the costs of glasses and/or contacts if they were needed.
That dichotomy now often causes great confusion when you make an appointment at your eye doctor. When making your appointment, the office is going to need to know which insurance, if you have both, you are going to be using for this particular visit.
Why does the office need to know in advance which insurance you are using?
The main reason is that the rules and sometimes the providers are different for each insurance plan. The vision plans often require the office to check on your availability for coverage and get pre-authorization for the visit BEFORE you get to the office. There are also differences in which providers within an office are in network for the insurance. For example, in some practices the optometrists might be in all the vision plans but the ophthalmologists might not in those plans. If you make an appointment with one of the ophthalmologists and tell the office you are using your health insurance, you can’t change your mind the day of the appointment and use your vision insurance instead.
There are also differences in what the insurance will cover as a reason for the exam. Vision insurance typically covers ONLY routine exams. Those are exams for which you are coming in specifically to get your vision, glasses and/or contact lens prescription checked and get an overall eye health screening. That means you CAN’T have a medical complaint about your eyes that you want the doctor to deal with. Eyes itchy? Need to use your medical/health insurance. Dry eyes? Need to use your medical/health insurance. Have a cataract? Glaucoma? Macular Degeneration? Need to use your medical/health insurance.
Why not just use your medical insurance all the time? That’s mostly because if you have no complaint at all your medical insurance won’t cover that visit (and “my vision is a little blurry” usually won’t cut it). There is one other issue and that is the refraction.
A refraction is when we check to see if you need a new eyeglass or contact lens prescription. For the most part, health insurance won’t cover the fee for the refraction, which is a procedure that is separate from your eye health exam. Your vision insurance will cover the refraction but not the exam if you are having a medical problem.
Here’s the real kicker. Your health insurance will cover your medical eye problems and your vision insurance will cover your refraction, BUT you can’t use both insurances at the same visit. It has to be one or the other. (Ridiculous right? I didn’t make the rules, just trying to abide by them.)
So, what are your choices if you have both a vision plan and health insurance? If you have a problem, you need to use your health insurance. If you want to have your eyes refracted so you can get new glasses at the same time you can either pay out of pocket for the refraction OR you can come back in for a second visit, using your vision plan to get a refraction and eye health screening exam so that the refraction gets covered. (Again - I didn’t invent these rules--I am just trying to help you navigate them.) If you don’t want to make two visits, then use your health insurance (with the appropriate complaint) and pay for the refraction and just use your vision insurance to help pay for the actual contacts or glasses you are going to buy.
If you have a question, it’s best to ask when you call the office to inquire about an appointment.
Article contributed by Dr. Brian Wnorowski, M.D.

The Centers for Disease Control estimates that around 2.8 million people in the United States suffer from a traumatic brain injury (TBI) every year, and vision can be affected. Concussions are a type of TBI.
The rate of childhood TBI visits to the emergency department more than doubled between 2001 and 2009, making children more likely than any other group to go to the ER with concussion symptoms.
It was once assumed that the hallmark of a concussion was a loss of consciousness. More recent evidence, however, does not support that. In fact, the majority of people diagnosed with a concussion do not experience any loss of consciousness. The most common immediate symptoms are amnesia and confusion.
There also are multiple visual symptoms that can occur with a concussion, either initially or during the recovery phase.
Visual symptoms after a concussion include:
-
Blurred vision.
-
Difficulty reading.
-
Double vision.
-
Light sensitivity.
-
Headaches accompanying visual tasks.
-
Loss of peripheral vision.
Most people with visual complaints after a concussion have 20/20 distance visual acuity, so more specific testing of near acuity, convergence amplitudes, ocular motility, and peripheral vision must be done.
In a study done at the Minds Matter Concussion Program at the Children's Hospital of Philadelphia, patients with a concussion diagnosis underwent extensive vision testing, which assessed symptoms, visual acuity, eye alignment, near point of convergence, vergence amplitude and facility, accommodative amplitude and facility, and saccadic eye movement speed and accuracy.
A total of 72 children (mean age 14.6 years) were examined, and 49 (68%) of those were found to have one or more vision symptoms after concussion. The most common problems were convergence insufficiency (47.2%); accommodative insufficiency (33.3%); saccadic dysfunction (30.5%); and accommodative infacility (11.1%). The investigators also found that 64% of the children with convergence insufficiency also had an accommodative disorder.
Difficulties with accommodation and convergence make it very hard to read for any length of time, with blurring and fatigue and then loss of concentration occurring after a fairly short period of reading time.
For the majority of people suffering a mild to moderate TBI, most of these symptoms resolve in one to three weeks but in some they can persist much longer.
If your visual symptoms after a concussion persist past three weeks, a visit with an eye care specialist is recommended. There may be several options to help improve the symptoms with either prescription eyeglasses or prisms to assist the two eyes to focus together.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
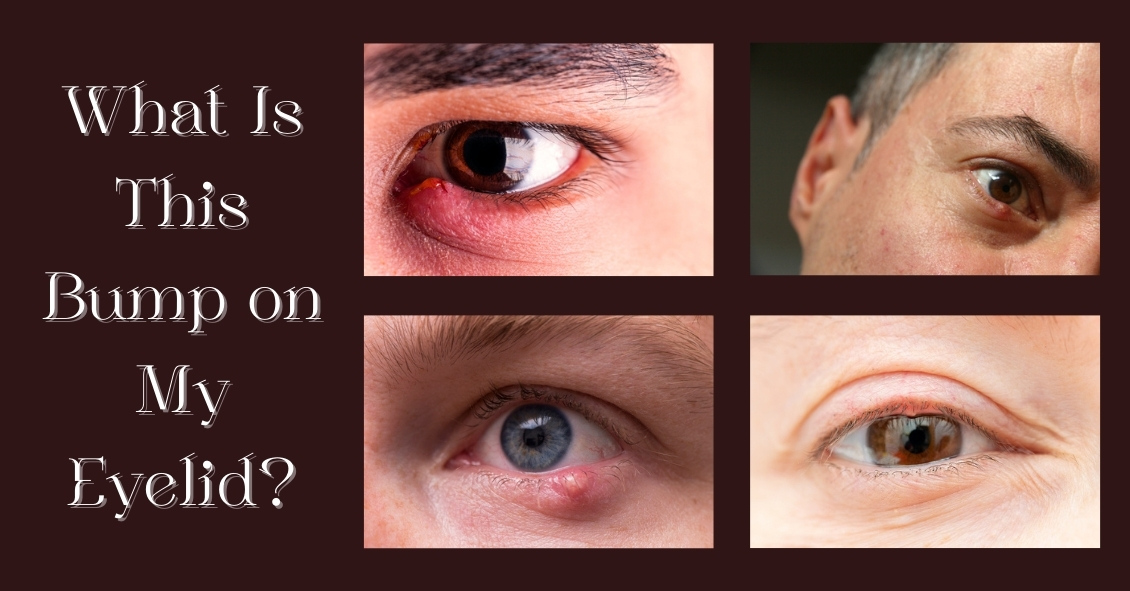
So you’re going about your day and notice a slight twinge when you blink. It starts off as a mild awareness, then proceeds to a painful feeling with every blink. You look in the mirror to see what could be causing it, and there you see a small red bump forming.
You decide to wait to see what happens and one of three things occurs. It might get bigger, redder, and more painful; it might shrink and goaway; or it might stay put, but it is no longer painful or growing in size. Let’s dive into one of the most common eye conditions we treat: hordeola (commonly known as “styes”) and chalazia.
Hordeola (or singular hordeolum), are infectious abscesses of the glands that line the eyelids. Bacteria that are naturally occurring on the eyelids and eyelashes can make their way into the gland and form what is essentially a pimple in the eyelid. If it goes untreated, hordeola can (rarely) lead to spreading of the infection throughout the eyelid (preseptal cellulitis) or even start to invade the orbit of the eye (orbital cellulitis). At that point, infection can spread to the brain and even be life-threatening and require hospitalization. Thankfully, it rarely gets to this point.
Treatment can consist of warm compresses, ointments, and oral antibiotics to kill the infection. Just like a pimple, it is not always necessary to be on antibiotics. It’s actually the warm compresses that do the most good. If you can get the gunk that is clogging the gland opening to thin out it will often just drain on its own without antibiotics. Sometimes, however, if the warm compresses alone aren’t working, and an antibiotic might be necessary. Don’t buy the over-the-counter ointment called “Stye.” It is not going to make it any better and could further clog the glands.
Chalazia (or chalazion singular) often start off as hordeola, but over time they become sterile, meaning non-infectious. Once the infection has cleared out, what is left behind is often what amounts to a marble-like lump in the eyelid. These are often more difficult to treat, as they no longer respond to antibiotics. If small enough, people can just leave them alone and see if they go away on their own. Larger ones, however, can be rather unsightly. If a chalazion no longer responds to warm compresses or ointments, we might treat it with steroid injection to shrink it, or it can be surgically removed.
We see these lumps and bumps on almost a daily basis in practice. Usually, they are very simple to treat and go away quickly.
Article contributed by Dr. Jonathan Gerard
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Itching, burning, watering, red, irritated, tired eyes... what is a person to do? These symptoms are classic signs of Dry Eye Syndrome (DES), which affects millions of adults and children.
What causes this? Dry eye syndrome can be brought on by many factors: aging, geographical location, lid hygiene, contact lens wear, medications, dehydration, etc. The lacrimal gland in the eye that produces tears, in a person over forty years old, starts slowly losing function. Females with hormonal changes have a higher incidence of DES (dry eye syndrome). Dry, arid climates or areas with high allergy rates tend to have higher incidences of DES as well. Another major cause is increased screentime--when we stare at a computer screen or phone, our blink reflex slows way down. A normal eye blinks 17,000 times per day, usually producing enough tears to be symptom free, if not contenting with other factors. But blink rates go way down while using screens.
Blepharities, a condition of the eyelids, can cause a dandruff-like situation for the eye, exacerbating a dry eye condition. Contact lenses can add to DES, so make sure you are in high oxygen contact lens material if you suffer from DES. Certain medications such as antihistamines, cholesterol and blood pressure meds, hormonal and birth control medications, can also cause symptoms of a dry eye. Check with your pharmacist if you are not sure if your medication could be contributing to the problem.
And finally, overall dehydration can cause DES. Some studies show we need 1/2 our body weight in ounces of water per day. For example, if you weigh 150 lbs, you need approximately 75 ounces of water per day to be fully hydrated. If you are not at that level, it could affect your eyes.
Treatment for DES is varied, but the main treatment is a tear supplement to replace the evaporated tears. These come in the form of topical ophthalmic artificial tears. Oral agents that can help are Omega 3 supplements such as fish oil or flax seed oil pills. They supplement the function of meibomian glands located at the lid margin. Ophthalmic gels used at night, as well as humidifiers, can help keep your eyes moisturized. Simply blinking hard more often can cause the lacrimal gland to produce more tears automatically.
For stubborn dry eyes, retaining tears on the eye can be aided by punctal plugs. They act like a stopper for a sink, and they are painless and can be inserted by your eye care practitioner in the office. Moisture chamber goggles can also be used in severe cases to hydrate the eyes with their body’s own natural humidity. This may sound far out but it gets the job done.
Being aware of the symptoms and treatments for dry eye syndrome can prevent frustration and allow your eyes to work more smoothly and efficiently in your daily routine. If your eyes feel dry as the Sahara or they water too much, know that help is on the way through proven techniques and products. You do not need to suffer needlessly in the case of Dry Eye Syndrome anymore. Make an appointment to talk with your eye doctor about the best treatments for you!
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
What Is Intraoperative Aberrometry?
Yes, that is a mouthful, but the concept isn’t quite as hard as the name.
An Intraoperative Aberrometer is an instrument we can use in the operating room to help us determine the correct power of the implant we put in your eye during cataract surgery.
Cataract surgery is the removal of the cloudy natural lens of your eye and the insertion of a new artificial lens inside your eye called an intraocular lens (IOL).
The cloudy cataract that we are removing has focusing power (think of a lens in a camera) and when that lens is removed, we need to insert an artificial lens in its place to replace that focusing power. The amount of focusing power the new IOL needs has to match the shape and curvature of your eye.
To determine what power of lens we select to put in your eye, we need to measure the shape and curvature of your eye prior to surgery. Once we get those measurements, we can plug those numbers into several different formulas to try and get the most accurate prediction of what power lens you need.
Overall, those measurements and formulas are very good at accurately predicting what power lens you should have. There are, however, several eye types where those measurements and formulas are less accurate at predicting the proper power of the replacement lens.
Long Eyes: People who are very nearsighted usually have eyes that are much longer than average. This adds some difficulty with the accuracy of both the measurements and the formulas. There are special formulas for long eyes but even those are less accurate than formulas for normal length eyes.
Short Eyes: People who are significantly farsighted tend to have shorter-than-normal eyes. Basically, the same issues hold true for them as the ones for longer eyes noted above.
Eyes with previous refractive surgery (LASIK, PRK, RK): These surgeries all change the normal shape of the cornea. This makes the formulas we use on eyes that have had previous surgery not work as well when the normal shape of the cornea has been altered.
This is where intraoperative aberrometry comes in. The machine takes the measurements that we do before surgery and then remeasures the eye while you are on the operating room table after the cataract is removed and before the new implant is placed inside the eye. It then presents the surgeon with the power of the implant that the aberrometer thinks is the correct one. Unfortunately, the power that the aberrometer selects isn’t always exactly right, but with the combination of the pre-surgery measurements and the intra-surgery measurements the overall accuracy is significantly enhanced.
The intraoperative aberrometry is also very helpful in choosing the power of specialty lenses like multi-focal and toric lenses.
We would encourage you to consider adding intraoperative aberrometry to your cataract surgery procedure if you have either a long or short eye (usually manifested as a high prescription in your glasses) or if you have had any previous refractive surgery.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Just like adults, children need to have their eyes examined. This need begins at birth and continues through adulthood.
Following are common recommendations for when a child needs to be screened, and what is looked for at each stage.
A child’s first eye exam should be done either right at or shortly after birth. This is especially true for children who were born prematurely and have a very low birth weight and may need to be given oxygen. This is mainly done to screen for a disease of the retina called retinopathy of prematurity (ROP), in which the retina does not develop properly as a result of the child receiving high levels of oxygen. Although rarer today due to the levels being monitored more closely, it is still a concern for premature babies.
The next time an eye exam is in order is around 6 months. At this stage, your pediatric eye doctor will check your child’s basic visual abilities by making them look at lights, respond to colors, and be able to follow a moving object.
Your child’s ocular alignment will also be measured to ensure that he or she does not have strabismus, a constant inward or outward turning of one or both eyes. Parents are encouraged to look for these symptoms at home because swift intervention with surgery to align the eyes at this stage is crucial for their ocular and visual development.
It is also imperative for parents and medical professionals to be on the lookout for retinoblastoma, a rare cancer of the eye that more commonly affects young children than adults. At home, this might show up in a photo taken with a flash, where the reflection in the pupil is white rather than red. Other symptoms can include eye pain, eyes not moving in the same direction, pupils always being wide open, and irises of different colors. While these symptoms can be caused by other things, having a doctor check them immediately is important because early treatment can save your child’s sight, but advanced cases can lead to vision loss and possibly death if the cancer spreads.
After the 6-month exam, I usually recommend another exam around age 5, then yearly afterward. There are several reasons for this gap. First, any parent with a 2- to 4-year-old knows that it’s difficult for them sit still for anything, let alone an eye exam. Trying to examine this young of a patient can be frustrating for the doctor, the parent, and the child. Nobody wins. By age 5, children are typically able to respond to questions and can (usually) concentrate on the task at hand. If necessary at this stage, their eyes will be measured for a prescription for glasses and checked for amblyopia, commonly known as a “lazy eye”. Detected early enough, amblyopia can be treated properly under close observation by the eye doctor.
The recommendations listed above are solely one doctor’s opinion of when children should have eye exams. The various medical bodies in pediatrics, ophthalmology, and optometry have different guidelines regarding exam frequency, but agree that while it is not essential that a healthy child’s eyes be examined every year, those with a personal or family history of inheritable eye disease should be followed more closely.
Article contributed by Dr. Jonathan Gerard
NOTE: Many eye doctors commonly like to have another exam around age 3, in order to make sure a pre-schooler's vision is developing correctly. Please go by what your trusted eye doctor advises and is comfortable with.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided on this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

"What are these weird floating things I started seeing?"
The spots, strings, or cobwebs that drift in and out of your vision are called “floaters,” and they are more prominent if you’re looking against a white background.
These floaters are tiny clumps of material floating inside the vitreous (jelly-like substance) that fills the inside of your eye. Floaters cast a shadow on the retina, which is the inner lining of the back of the eye that relays images to the brain.
As you get older, the vitreous gel pulls away from the retina and the traction on the retina causes flashing lights. These flashes can then occur for months. Once the vitreous gel completely separates from the back wall of the eye, you then have a posterior vitreous detachment (PVD), which is a common cause of new onset of floaters.
This condition is more common in people who:
- Are nearsighted.
- Are aphakic (absence of the lens of the eye).
- Have past trauma to the eye.
- Have had inflammation in the eye.
When a posterior vitreous detachment occurs, there is a concern that it can cause a retinal tear.
Symptoms of a retinal tear include:
- Sudden increase in number of floaters that are persistent and don't resolve.
- Increase in flashes.
- A shadow covering your side vision, or a decrease in vision.
In general, posterior vitreous detachment is unlikely to progress to a retinal detachment. Only about 15 percent of people with PVD develop a retinal tear.
If left untreated, approximately 40 percent of people with a symptomatic retinal tear will progress into a retinal detachment – and a retinal detachment needs prompt treatment to prevent vision loss.
Generally, most people become accustomed to the floaters in their eyes.
Surgery can be performed to remove the vitreous gel but there is no guarantee that all the floaters will be removed. And for most people, the risk of surgery is greater than the nuisance that the floaters present.
Similarly, there is a laser procedure that breaks the floaters up into smaller pieces in hopes of making them less noticeable. However, this is not a recognized standard treatment and it is not widely practiced.
In general, the usual recommendation for floaters and PVD is observation by an eye care specialist.
Article contributed by Jane Pan M.D.
The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ. This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician.

There are many opinions on the topic of texting and driving. The goal of this blog post is to explore the effects on vision during texting.
So, from a visual perspective, why does texting make you more likely to crash? The problem lies in distraction from driving. For example, it takes a fast texter approximately 20 seconds to read and reply to a text. At 55 mph on the highway, a driver glances away from the road for approximately one-third of a mile. When the driver is focusing on their screen, this essentially gives the driver tunnel vision, causing the visual system to essentially use peripheral vision for driving. Your central vision is used to detect depth perception, detail, and colors such as red or green. So when texting, your depth perception, or 3-D vision, is altered and if cars are stopped ahead or closing in rapidly, it's not as easily detected. Colors, such as red brake lights or traffic signals, are not as easily noticed.
Next time you encounter situations with texting and driving, know that the visual system was designed to perform advanced visual perception while using central vision. This includes detail vision, depth perception, and color vision....all of which are placed on hold while texting and driving.
For more information on texting and driving see:
US Dept. of Transportation
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Despite requests that patients bring their current glasses to their office visit, many show up without them.
Sometimes it’s an oversight: “I was rushing to get here and forgot them”; “I left them in the car”; “I picked up my wife’s glasses instead of mine by mistake.” Doctors have heard them all.
Sometimes it is unavoidable: “I lost them”; “They were stolen”; “I ran them over with the car”; “I left them on the roof of the car and drove away and now they are gone.”
Frequently, however, it’s intentional. There is a perception by some people that if they don’t like their current glasses or feel like they are not working well for them that they are better off having their eye doctor start from scratch. “Why would I want the doctor to utilize a pair of glasses I’m not happy with as a basis or starting point for my next pair of glasses?”
But bringing your glasses to an appointment is important.
There are two main reasons for eye care professionals to know what your last pair of glasses were.
The first is to see what type of glasses they are and how you see out of them. Are they just distance? Just reading? A bifocal? A trifocal? A progressive?
Even if you feel they aren’t working for you, it is essential for doctors to know the type of lens you had previously. It is also important to know how you see out of them and what the previous prescription was. This can help eye care professionals determine a new prescription that will work better for you.
The second reason doctors like to know what was in your last pair of glasses is that the majority of people who wear eyeglasses have some degree of astigmatism in their eyeglass prescription.
A significant change in either the amount or axis of the astigmatism correction from one pair of glasses to the next is often not tolerated well, especially in adults. If there is too much change from the previous prescription, many people experience a pulling sensation in their eyes when they wear the new glasses. It can cause symptoms of eye strain, headaches, and distortion, making flat objects like a table look like they are slanted.
Many of the problems that occur when we try to give someone a new eyeglass prescription could be avoided if doctors knew the last prescription and how you did with it.
Anytime you are going to the eye doctor, it is essential to bring your most current pair of glasses with you to the exam--whether you love them or hate them!
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided on this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Did you know that having one's eyes tested can reveal symptoms of ADHD (Attention Deficit Hyperactivity Disorder)? ADHD is a set of symptoms that includes trouble with focus, overactivity, and behavioral control. It is estimated that one in five people has some sort of ADHD.
ADHD is a condition that has multiple symptoms and it can affect any age, though commonly it affects children. There is difficulty with visual processing, which includes doubling letters, reversing letters, and jumping words and lines of print.
Eye examinations are a crucial part of the diagnosis of ADHD. Proper visual function can be assessed through a thorough eye exam. During the exam, visual complaints, focusing, and processing can be assessed to rule out ADHD.
When glasses are prescribed for an patient with ADHD, prescribing the correct type of lens is vital. Many patients benefit from an anti-glare/anti-reflective or AR treatment on their lenses. This cuts unnecessary light from entering the eye, making visual processing easier.
In some cases, it is discovered that the person has a non-ocular visual processing problem. This simply means that their eyes have little or nothing to do with the symptoms of ADHD. This gives valuable information to the health care provider that is managing the patient and suggests more non-ocular testing for a compete diagnosis.
ADHD is very common, and the great news is that there are multiple treatment options. Many resources for help are available on the Internet and through health care channels.
Having an eye exam should be one of the first items on the checklist if you are suspicious about ADHD because valuable information on visual processing can be gained.
For more resources see these websites:
National Institute of Mental Health, www.nimh.nih.gov/
American Optometric Association, AOA.org
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.